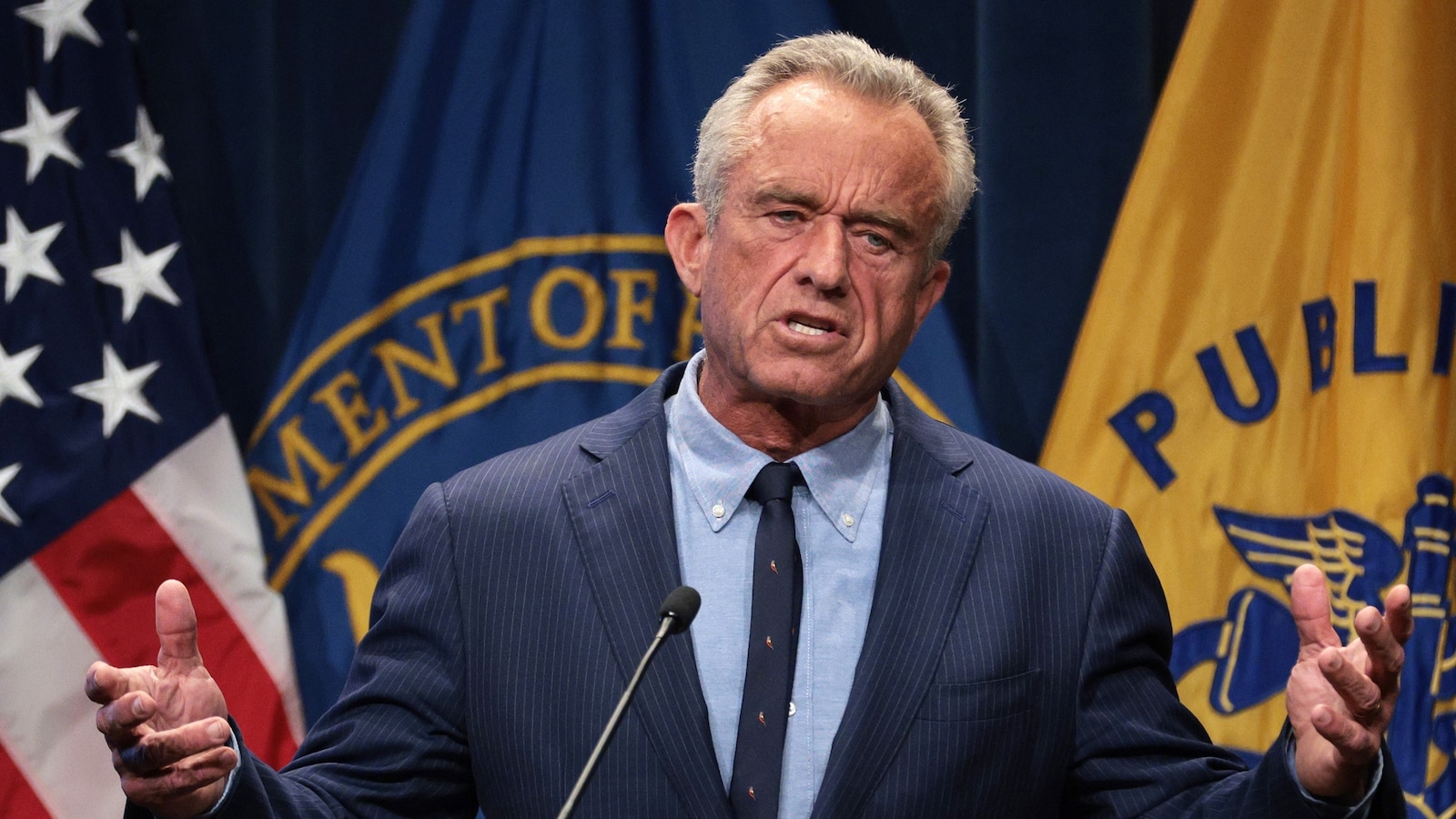


























The head of the US Department of Health and Human Services, Robert F. Kennedy Jr., recently announced significant funding cuts for mRNA vaccine development, claiming these vaccines are ineffective against respiratory diseases such as COVID-19 and flu. This declaration, which includes a reduction of $500 million in funding, contradicts prevailing scientific evidence demonstrating that many mRNA vaccines are effective, often outperforming traditional vaccine types.
In his announcement, Kennedy stated, “These vaccines fail to protect effectively against upper respiratory infections like COVID and flu.” He indicated that the agency would redirect funding towards “safer, broader vaccine platforms that remain effective even as viruses mutate.” This assertion raises concerns, as the effectiveness of vaccines varies significantly based on the nature of the viruses they target, rather than the type of vaccine itself.
Understanding Vaccine Effectiveness
Different vaccine types exist, including live viruses, killed viruses, genetically engineered viral shells, single viral proteins, and mRNAs coding for viral proteins. For example, the MMR vaccine demonstrates high effectiveness, reaching nearly 100% in preventing measles outbreaks when vaccination rates exceed 90% in a population. This success is largely attributed to the measles virus’s stability, which remains relatively unchanged over time.
Conversely, respiratory viruses such as those causing colds and flu infect the cells in the nose and throat, making it challenging to generate sufficient levels of effective antibodies in these areas. The rapid mutation rates of cold, flu, and COVID-19 viruses further complicate the ability to achieve lasting immunity. Consequently, no flu or COVID-19 vaccine provides the same lifelong protection as the measles component of the MMR vaccine.
Despite Kennedy’s claims, mRNA vaccines have demonstrated substantial efficacy. Some mRNA COVID-19 vaccines have shown effectiveness rates exceeding 90% against symptomatic infections, with even higher protection against severe disease. In comparison, the effectiveness of non-mRNA vaccines for annual flu varies between 20% and 60%. A recent trial also revealed that a combined COVID-flu mRNA vaccine outperformed existing non-mRNA flu vaccines in individuals aged over 50, who are particularly vulnerable.
Evaluating Claims on Vaccine Platforms
Kennedy’s assertion that other vaccine types are more likely to remain effective as viruses mutate points to the concept of “universal vaccines.” These aim to provide protection against all variants of a particular virus, such as all flu viruses or all coronaviruses, by targeting stable parts of the virus. However, achieving this goal presents significant challenges, as viruses often conceal their stable components beneath mutable ones.
Despite decades of efforts, the development of effective universal vaccines remains elusive. Therefore, shifting substantial funding towards these initiatives could hinder progress in addressing current health challenges. Notably, mRNA technology itself has been employed in experimental universal vaccine efforts, further undermining Kennedy’s claims.
While efficacy is crucial, other factors such as safety, cost, and the speed of vaccine development are equally important. In these areas, mRNA technology offers notable advantages. It is generally safer than vaccines comprising live viruses, less expensive than those based on single viral proteins, and can be developed much faster—an essential factor in responding to rapidly changing respiratory viruses during a pandemic.
The funding cuts announced by Kennedy could slow mRNA vaccine development, potentially deterring companies from investing in this promising approach. The implications of this decision extend beyond immediate vaccine efficacy; they could impact the broader landscape of vaccine development and public health responses to emerging infectious diseases.